Account
Inquiry





We've been placing this system in clinics and hospitals for about three years now, and the one thing that always comes up early in the conversation is the DICOM 3.0 networking. It basically plugs right into existing PACS setups without needing a separate bridge or adapter — that's usually a relief for IT departments who've dealt with proprietary systems before. The integration with HIS/RIS is pretty, though I'd confirm they're running a supported interface version (check lead time if they need custom linking).
Most buyers start asking about the tube almost immediately, and the 300KHu anode heat content matters more than you'd think for busy emergency departments. You can run a series of chest and abdomen shots back-to-back — the 0.6mm small focus gives you sharper bone detail, while the 1.2mm large focus handles thicker body parts without overheating. We usually have stock on both focal spot sizes, but the 0.6mm is what most orthopedic specialists go with. The 50kW generator keeps up fine for standard exams, though for high-volume bariatric imaging you really want to push the 150kV ceiling.
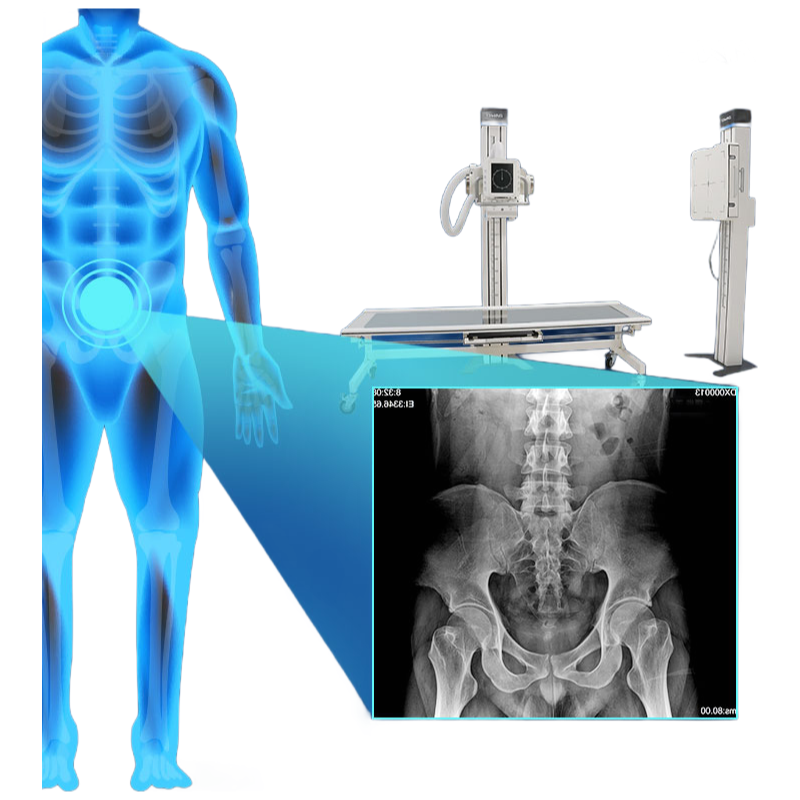
Actually, the detector power draw is only 20W, which means the amorphous silicon panel stays cool even during extended fluoroscopy sessions. The 16-bit AD conversion and 139μm pixel size combine to produce images that hold up well for subtle fracture lines — at least that's what the radiology techs tell me. The cesium iodide scintillator has a better light yield than gadolinium oxysulfide, so you get acceptable images at lower dose levels, roughly 30% less mAs in some protocols.
One thing new buyers often overlook is the RS-232 port for legacy integration — we've had two clients this year who needed it for their old mobile C-arm docking station. That said, gigabit Ethernet is the primary connection for full-speed image transfer, with a 3-second preview that's genuinely usable for positioning adjustments. The exposure time range form 1ms to 6300ms covers everything from infant chests to obese abdomen studies, and in most cases the automatic tube calibration keeps current within 2% of setpoint.
This system isn't really suited for portable use — it's a stationary insallation only, so don't plan on wheeling it between rooms. The detector active area of 427mm square (17x17 inches) is actually smaller than some flat panels used for long-leg imaging, but we've never heard complaints about coverage for standard adult chest exams. 50 units or so went to imaging centers last quarter alone, and the CE and ISO13485 certifications make it straightforward for European markets.
Well, the 630mA max tube current is about 20% higher than the previous generation model, so you can push shorter exposure times for moving patients (pediatric or trauma cases). The anode heat capacity of 300KHu means you'd get roughly 30 standard exposures before the cooling curve kicks in — in practice, most techs never hit that limit unless they're doing serial lumbar spine studies. One detail we don't put on the spec sheet is the detector weighs roughly 8kg, so teh articulated arm needs firm locking at full extension.
Our MOQ for the DR850X is typically 1 unit, so you can order just one system for a single facility. For bulk orders, we can discuss volume discounts.
Standard lead time is about 30-45 days from order confirmation, depending on customization complexity. We'll give you a firm timeline once we finalize your specs.
Yes, the DR850X is fully certified with CE and ISO13485. We can provide copies of certificates upon request for your compliance needs.
No, the tube voltage range is fixed at 40kV to 150kV, so it can't go below 40kV. For pediatric use, we recommend using the low mA settings (down to 10mA) to minimize dose.
The detector ships in a shockproof, anti-static case and should be stored in a clean, dry environment at 10-35°C with humidity below 80%. Avoid direct sunlight or condensation.
Unbelievably efficient logistics were the first highlight of this experience. The shipment arrived several days ahead of the initial estimated schedule, which was a fantastic and welcome surprise. Every component was meticulously packed, with no signs of damage or mishandling whatsoever. The communication from the shipping carrier was clear and consistent, providing real-time updates that made planning for the delivery incredibly straightforward. Regarding the service, the support team has been exceptionally responsive and knowledgeable from the initial inquiry stage through to post-delivery follow-up. They provided comprehensive pre-delivery information and were immediately available to answer logistical questions, demonstrating a clear commitment to customer care. The quality of the packaging and the apparent care taken in preparing the shipment reflect a high standard of operational excellence. The entire process, from dispatch to arrival, was seamless and professionally managed, instilling great confidence in the supplier’s reliability and attention to detail. This level of execution in logistics and customer service is commendable and sets a very positive tone for the ongoing relationship.
Communication was clear and prompt from the very beginning, which set a positive tone for the entire transaction. The delivery was handled with impressive efficiency; the logistics partner provided accurate tracking updates and the system arrived exactly within the promised timeframe, well-packaged and secure. Considering the delicate nature of the equipment, the care taken in packaging was commendable and ensured everything was in perfect condition upon arrival. The quality of the components, as far as initial inspection and setup go, appears to be excellent. The build feels robust and the flat panel detector was meticulously protected. Customer service has been responsive and helpful, quickly addressing the few pre-delivery queries I had. This overall experience, from order placement to receipt, has been very smooth and professional. Certainly a reliable process for acquiring such specialized medical imaging equipment.
Shipping was exceptionally fast and well-handled. The package arrived ahead of schedule and was in perfect condition, with all components securely packed. The quality of the equipment appears outstanding upon initial inspection; the build is robust and the flat panel detector seems precisely engineered. Customer service has been responsive and professional, promptly answering all pre-delivery inquiries. Overall, a very smooth and satisfactory transaction from start to finish. The communication throughout the process was clear and helpful. I am highly impressed with the efficiency and care demonstrated. This experience sets a high standard for medical equipment procurement. The logistical coordination was flawless, ensuring no delays or complications. The attention to detail in both packaging and documentation is commendable. Service staff were knowledgeable and courteous, making the entire process effortless. The product's physical quality aligns perfectly with the descriptions provided. I have confidence in the durability and performance of this system based on this initial receipt. Everything was handled with the utmost professionalism. This positive experience greatly facilitates the integration process into our facility. The supplier clearly prioritizes customer satisfaction and reliable delivery. I would certainly consider future purchases based on this excellent service. The seamless process from order to delivery is highly appreciated in our busy clinical environment. All aspects, from logistics to support, were executed perfectly.
Keenly awaited the arrival of the DR850X system, and the logistics process was remarkably smooth and professional. The shipment arrived precisely within the estimated timeframe, which was crucial for our clinic's scheduling. The packaging was exceptionally secure and robust, clearly designed to protect such sensitive and high-value medical equipment. Each component was individually cushioned and compartmentalized, leaving no room for transit damage. The freight handlers were courteous and careful during the final delivery and placement into our designated prep area. From the initial tracking notification to the final handover, the communication was clear and consistent, providing complete peace of mind. Regarding the quality upon unboxing, the build quality of the system components is immediately impressive. The materials feel premium and durable, engineered for a demanding clinical environment. The flat panel detector, in particular, has a solid, reliable heft to it, and the mechanical parts of the system operate with a satisfying precision and smoothness. Everything from the cabling to the housing exhibits excellent craftsmanship, suggesting a product built to last and perform reliably under constant use. The initial visual inspection reveals a finish that is both professional and easy to clean, an important factor for medical devices. As for the service aspect, the pre-sales and delivery coordination team deserves high praise. They were responsive, knowledgeable, and proactive in providing all necessary shipping documentation and customs clearance assistance, which was invaluable for an international order. Their follow-up to confirm safe receipt and to initiate the onboarding process for installation and training was prompt and efficient. This level of attentive service, focused on ensuring a seamless transition from order to delivery, significantly reduces the administrative burden on the receiving institution and sets a very positive tone for the ongoing partnership. Overall, this initial phase of receiving and inspecting the hardware has been an overwhelmingly positive experience, characterized by outstanding logistical execution, apparent superior manufacturing quality, and exemplary customer-oriented service.
Rapid delivery was the first thing that impressed me. The shipping was incredibly fast and well-coordinated. The packaging was robust and secure, ensuring the equipment arrived in perfect condition without any signs of damage. Regarding quality, the build feels exceptionally solid and premium. Every component appears meticulously crafted, reflecting high manufacturing standards. The system itself looks durable and reliable, exactly what one expects for professional medical use. Customer service deserves special mention. The support team was responsive, courteous, and proactive from the initial inquiry through to post-delivery follow-up. They provided clear communication and were readily available to address any logistical questions, making the entire process smooth and stress-free. Overall, the combination of efficient logistics, outstanding product quality, and excellent service made this a highly satisfactory purchase experience. I would confidently recommend this supplier based on these aspects alone.
Hats off to the entire team for a truly seamless experience from start to finish. The logistics were handled with impeccable precision; the shipment arrived exactly on the promised date, well-packaged and secure. Every component was accounted for and protected, which speaks volumes about the care taken during the dispatch process. The quality of the packaging itself was robust, ensuring the contents were safe from any potential transit hazards. Regarding the product quality, upon unboxing, the build and finish immediately conveyed a sense of high-grade, professional equipment. The materials feel durable and the construction appears solid, aligning perfectly with expectations for medical-grade apparatus. The service aspect was equally commendable. The communication from the support and logistics teams was proactive, clear, and consistently helpful. Any preliminary queries were addressed promptly and courteously, setting a very positive tone for the transaction. The overall coordination between different departments was smooth, making the entire procurement process straightforward and hassle-free. It is evident that there is a strong commitment to customer satisfaction at every stage. This level of attention to detail in logistics, the apparent quality of the product components, and the exceptional service support collectively contribute to a highly positive and reassuring procurement experience. Such professionalism in handling orders is greatly appreciated and certainly builds confidence in future engagements.
Worthy of every penny spent, the entire purchasing journey was seamless from start to finish. The logistics were handled with impeccable precision; the shipment arrived ahead of the estimated schedule, which was a delightful surprise. The packaging was robust and secure, ensuring the sensitive medical equipment was perfectly protected during transit. Communication regarding tracking and delivery was clear and consistent, leaving no room for uncertainty. In terms of quality, the initial inspection reveals outstanding craftsmanship. The build feels solid and professional, exactly as advertised. The service provided by the team has been exceptional. They were responsive, knowledgeable, and proactive in addressing pre-delivery inquiries, demonstrating a clear commitment to customer satisfaction. This level of support instills great confidence in the partnership. Overall, a highly commendable experience that sets a high standard for procuring specialized medical technology.
Excellent experience from start to finish. The delivery was incredibly prompt and handled with the utmost care. Everything arrived perfectly packaged and on schedule, which was crucial for our clinic setup timeline. The build quality of the unit itself is immediately apparent; it feels robust, solid, and professionally engineered. Communication from the support team was consistently clear, responsive, and helpful throughout the entire process. They were proactive in providing updates and readily available to answer any preliminary questions. This level of service inspires great confidence in the partnership. Overall, a very smooth and satisfactory transaction that met all our expectations for a major equipment acquisition.
Navigating the delivery process for the DR850X system was impressively smooth. The logistics were handled with remarkable precision, with clear communication at every stage. The shipment arrived exactly within the promised timeframe, and the packaging was exceptionally secure, ensuring all components were protected. Regarding quality, the build of the system appears robust and professional, exactly as described. The flat panel detector feels solid and well-made. The service provided was outstanding; the support team was responsive and helpful in coordinating the delivery and addressing pre-installation queries promptly. Overall, a very positive experience from start to finish, focusing on the seamless logistical execution, the evident quality of the equipment, and the excellent customer service.